
People with severe mental ill health are being routinely ‘warehoused’ in locked, private wards hundreds of miles away for want of NHS care closer to home, an investigation reveals.
Research by The Doctor magazine has found that five million people live in CCG (clinical commissioning group) areas in England with no NHS wards at all for mental health rehabilitation, a service that helps people with severe illness get their lives back on track.
While some CCGs pay for such beds in the NHS, most depend heavily on private hospitals and care homes – and increasingly so, according to data obtained by our Freedom of Information requests.
Hundreds of private beds are hours and hours away from patients’ homes, analysis of 2,600 journeys found. Seven hundred are sold to CCGs as ‘locked rehab’, a type not recognised in NHS guidance – raising concerns about patient care and human rights.
Stays on private wards last twice as long as in the NHS, doubling the expense, the pain of separation from families, and frustrating efforts by local staff to bring people back home.
‘Extremely disturbing’
The findings have alarmed senior psychiatrists. ‘Out-of-area placements in rehabilitation wards have become endemic in the NHS,’ says consultant psychiatrist Andrew Molodynski, mental health policy lead for the BMA consultants committee.
‘Warehousing unwell people in locked wards far from home goes against the very nature of mental health rehab – to help them reintegrate back into society.’ Chair of the rehabilitation faculty at the Royal College of Psychiatrists Raj Mohan describes the findings as ‘extremely disturbing’. ‘We are failing people who need rehabilitation care,’ he adds.
Private beds
Mental health rehabilitation is supposed to help people regain independence. It unpicks and treats the mesh of social and health issues, which can arise with serious illness, trapping some in cycles of short stays on acute wards, where they’re only patched up. It takes time. Stays last six months to a year, sometimes longer. Patients often start in ‘high-intensity’ wards.
Most are detained under the Mental Health Act to keep them safe. As they improve, they’re ‘stepped down’ to less secure units, before being settled back home by community teams, working closely with staff on the wards. Most return to supported accommodation.
This pattern of treatment or ‘care pathway’ has, however, become badly fractured in parts of England where permanent NHS mental health rehabilitation wards are closed and replaced by private beds far from home.
Many of these private placements are arranged ad hoc by CCGs, as ‘spot purchases’. This use of spot-purchased beds – especially in areas with no services of their own – raises an obvious concern: who checks on the care of these patients when they’re away? Some trusts don’t even know where patients in their patches are sent.
Two, Birmingham and Solihull Mental Health NHS Foundation Trust and Dorset HealthCare University NHS Foundation Trust, held no records for people in ‘spot-purchased’ beds, they said. It was their CCGs, the bodies responsible for commissioning – not providing clinical care – which knew about them.
Far from loved ones
 Dr Molodynski
Dr Molodynski
The BMA’s Dr Molodynski points to known risks of sending patients to wards far from their families and close clinical supervision.
‘As seen in the extreme cases of Whorlton Hall and Winterbourne, the “cut-off” nature of these institutions can be a breeding ground for the development of harsh and abusive cultures.’
The Doctor identified three instances of patients sent to Whorlton Hall, the private hospital closed after Panorama exposed horrific abuse of patients by staff in its investigation.
In all three cases we identified, patients came from areas more than 100 miles away. The human cost of poor care in mental health rehab is well known to David Shiers, a retired GP, who campaigns for better mental health rehab following the awful early experience of his daughter Mary (see ‘Road to recovery’ below).
Mary’s schizophrenia transformed her from a normal teenager into a ‘terrified young woman’, he says. She was admitted to an adult asylum before being offered a place 50 miles away.
Her family fought for years before a local service was opened. It transformed Mary’s life but was closed after she moved out. ‘Where would Mary be if she didn’t have parents who were health professionals?’ Dr Shiers asks.
Greater costs
While the Shiers’ battle is past, many other families face similar or worse problems, The Doctor’s research indicates. The replacement of local wards with ad hoc out-of-area beds has not just had a human cost.
It’s costly to the NHS, too. An extensive study of mental health rehabilitation by the CQC (Care Quality Commission) last year found that stays in private beds cost twice as much as in the NHS because they last twice as long. It found the annual cost of rehab was £535m and that private beds were on average 30 miles away from patients’ homes but just nine miles away in the NHS. The NHS has taken steps since the CQC report.
NHS Improvement launched a ‘Getting It Right First Time’ programme for mental health rehab last year, led by respected London consultant psychiatrist Sridevi Kalidindi. It helps trusts in England to improve. ‘This is an enormous, long overdue opportunity to upgrade rehabilitation services nationally,’ she says.
For its part, the CQC tweaked inspections. It now checks that the right staff with the right skills are on wards and that they’re geared towards helping people leave; not acting as expensive hotels.
Missed abuse
Inspections are far from perfect, however. They failed to pick up abuse at Whorlton Hall during checks in 2018, a missed opportunity for which it has apologised. It’s hard to ‘get under the skin’ of places where people are placed for long periods far from home, CQC deputy chief inspector of hospitals Paul Lelliott admitted last month.
CCGs, however, seem split about the CQC’s findings on costs. Sandwell and West Birmingham CCG, which commissions no inpatient rehab for its half a million population, ‘contests’ the view that private beds are more costly. Its patients are ‘tracked’ in their private beds by the CCG’s own mental health clinicians, a spokesperson says. They ‘challenge the local NHS provider to recover people in a timely way to their own local community solution’.
Worsening situation
Sandwell and West Birmingham has spent £20m on private beds in the past three years. More than 100 were out of area, one hour’s drive away, on average. NHS commissioners for the Lancashire and South Cumbria Integrated Care System, however, admit that its service ‘does not always represent best value for money or best experience for patients or their families’.
One of its CCGs, Greater Preston, spent £10.3m on private beds up to 229 miles away. The care system is talking to Lancashire Care NHS Foundation Trust about opening wards for ‘quality, value for money and less restrictive post-hospital care, closer to home for patients’, a spokesperson says.
The investigation, however, points to a worsening picture for mental health rehab across England as parts of the NHS try to improve.
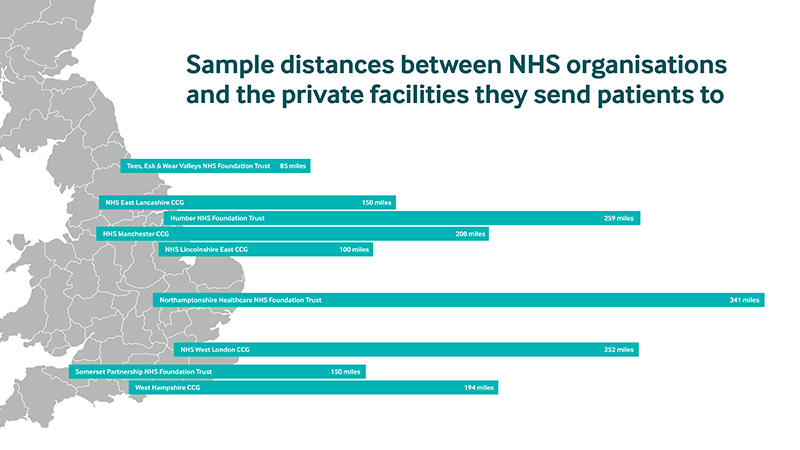
It found patients were sent to private beds up to 341 miles away, leaving families and NHS staff with a five-and-a-half hour drive for a single visit. Hospitals in Northamptonshire sent patients to Scotland. Devon bought beds in Harrogate, Yorkshire.
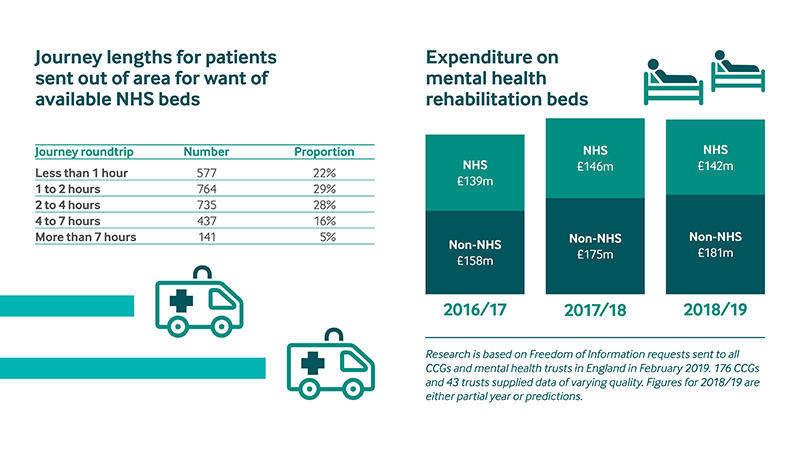
More than half of beds were over an hour’s drive away; one in five were more than 100 miles from home. 90 per cent were in the more costly private sector. CCG figures are also increasingly reliant on private providers, we found. The NHS spent 56 per cent of its rehab budget on private beds last year up from 53 per cent in 2016/17. The number of beds bought from private providers jumped 10 per cent in the same period. And the appetite for growth in the private sector shows little sign of receding.
Private beneficiaries
Market analysts speak of ‘sharp’ revenue rises for private mental health services. They swelled a ‘remarkable’ 12 per cent in 2015, followed by 4 per cent in 2016, according to analysts, LaingBuisson. 87 per cent of independent sector mental health services income is from the NHS, the CMA (Competition and Markets Authority) reported in late 2017.
Not all rehab psychiatrists are opposed to the involvement of private providers in their patients’ care. But many are worried about services’ exposure to market forces, something greatly increased by the Health and Social Care Act of 2012. Some damage has already been done by this exposure.
There’s the proliferation of out-of-area beds in the private sector and the use of ‘locked rehab’ wards by CCGs which have no or too few beds of their own. Almost all locked rehab wards (97 per cent) are run by private hospitals, the CMA report says. The Doctor investigation found 700 were used by the NHS last year.
The trouble with locked rehab wards is that they are not specified in NHS guidance, so doctors can’t be sure what they’re like. They’re thought to resemble the ‘high dependency’ wards of the NHS rehabilitation ‘care pathway’ – wards which patients need special permission to leave.
This means people can be locked in for their whole stay – with no chance of more freedom as their illness improves – a key principle of rehabilitation. ‘No mental health service should be specified by the locksmith,’ the RCPsych’s Dr Mohan, says. ‘Restrictions on freedom should be short, determined by people’s need, and stopped as soon as is feasible.’
‘This is a human rights issue,’ says University College of London professor of psychiatry, Helen Killaspy. ‘Why should you be sent away just because you’ve been dealt this unlucky hand of cards that gives you complex psychosis? It’s just wrong that you should be marginalised, shuffled off, even if it is to a comfortable hospital room in the private sector – people don’t need to be there for as long as they are staying.
They don’t need to be treated out of area and they don’t need to be always locked up.’ The BMA’s Dr Molodynski says the Government should ‘get a grip’ on the worrying practice of patients locked up in the ‘gilded cages’ of unplanned and expensive ad hoc placements.
‘There are no positives at all here for patients, families, care services, or the public purse – quite the opposite. We need to ensure that care is available closer to home to give patients the best possible chance of recovery and reintegration.’
Road to recovery: a family’s fight for its daughter’s life

It’s some time since we first shared a personal view about our daughter’s (pictured above, centre) early experience of care for schizophrenia and how we felt the NHS had failed her (Who Cares? BMJ 1998) This severe illness transformed Mary from a normal 16-year-old schoolgirl into a terrified young woman, unable to think, communicate or take part in life.
‘First came a year of appointments in children’s clinics and the apologetic assurance: adult services would be ‘more into psychosis’.
Support at home became unsustainable. Mary was admitted to an acute adult ward, then to a rehabilitation unit in a local asylum, an eight-bed Dickensian dormitory. She was drugged, lost in her own world, barely acknowledging us.
There was nothing to do on her ward, nowhere to go. Just older patients wandering long, dismal corridors, a foresight of Mary’s future. A strength of rock bottom is that you cannot sink lower. But with support from her excellent psychiatrist we fought back. We asked our local health authority: was her care satisfactory, given that numerous agencies had catalogued serious unmet need? Providing a bed met its responsibility, came the reply.
After months of fruitless exchanges we contacted the regional health authority. Its mental health lead called. He listened. He saw where Mary was staying. He agreed this was not meeting her needs. Our local health authority then offered Mary a choice of five community rehabilitation services, but all more than 50 miles away.
With Mary’s psychiatrist we challenged again: had they considered the effect of separating Mary from her family and home environment? Why weren’t there local services? After two long years of pressure, health and social services finally commissioned a local rehabilitation service in the community for Mary and 16 other young people.
It was a modern home in the real world. She had her own room, her own pictures. She listened to her own music and liked being with other young people. Within weeks, Mary began to improve and to find her identity. There were activities, focusing on her strengths, not her weaknesses. She tentatively explored her new surroundings, went to a local college, went shopping. She began to enjoy family activities. Free from the ward regimen, her days took on meaning.
After 18 months, Mary successfully moved on to a residential care home. The community rehab service closed soon afterwards; the old asylum became a smart housing estate. Now in her 40s, Mary lives in an excellent residential care home, free of symptoms of psychosis but still requiring support for daily activities. Her world revolves around the town she grew up in. She lives for today, takes pride in her appearance.
We’re so proud she has come through. But where would Mary be now if she didn’t have parents who were health professionals? If she hadn’t had a brave and principled psychiatrist or a mental health lead with skills, experience and compassion?
David Shiers is a retired GP (pictured above, right). Ann Shiers is a retired district nurse (pictured above, left).
Dr Shiers is: an adviser to the NICE (The National Institute for Health and Care Excellence) centre for guidelines and a member of the NICE guideline development group for rehabilitation in adults with complex psychosis and related severe mental health conditions; board member of the NCCMH (National Collaborating Centre for Mental Health); and his views are personal and not those of NICE or NCCMH.