
The closest Lee Snowball came to home comforts for 17 years were a makeshift bed in a lift shaft, bottles of milk pinched from estate doorways, and a stolen sofa in an abandoned garage.
Life was ‘tough and lonely’ – sometimes he had to fight, literally, to survive those long nights.
In 2016, those thousands of nights sleeping rough, or staying with friends, had taken their toll on his body and significant surgery was required to correct a bowed knee and some other, resulting, issues.
Vicious cycle
After successful surgery Mr Snowball faced a return to sleeping in the park near his godmother’s house or taking shelter in the cubbyholes and rabbit warrens of a North London housing estate – on crutches, with a large, healing wound.
However, medically fit for discharge is surely not equivalent to fit to be discharged to the streets? As a Department of Health study published in 2010 said: ‘Clearly, living conditions on the streets are not conducive to recovery from poor health; neither do hostels provide all elements of a good environment for recovery.’
Readmission and complications would have been almost inevitable in Mr Snowball’s case. He faced becoming a victim of a vicious cycle, a spiralling relationship between ill health and homelessness.
His is just one story behind a growing avalanche of statistics captured by The Doctor – with the interaction between homeless patients and the NHS rocketing as the cuts to services and stored up trauma of austerity policies bite hard across the country.
Living conditions on the streets are not conducive to recovery from poor health.
The walking wounded
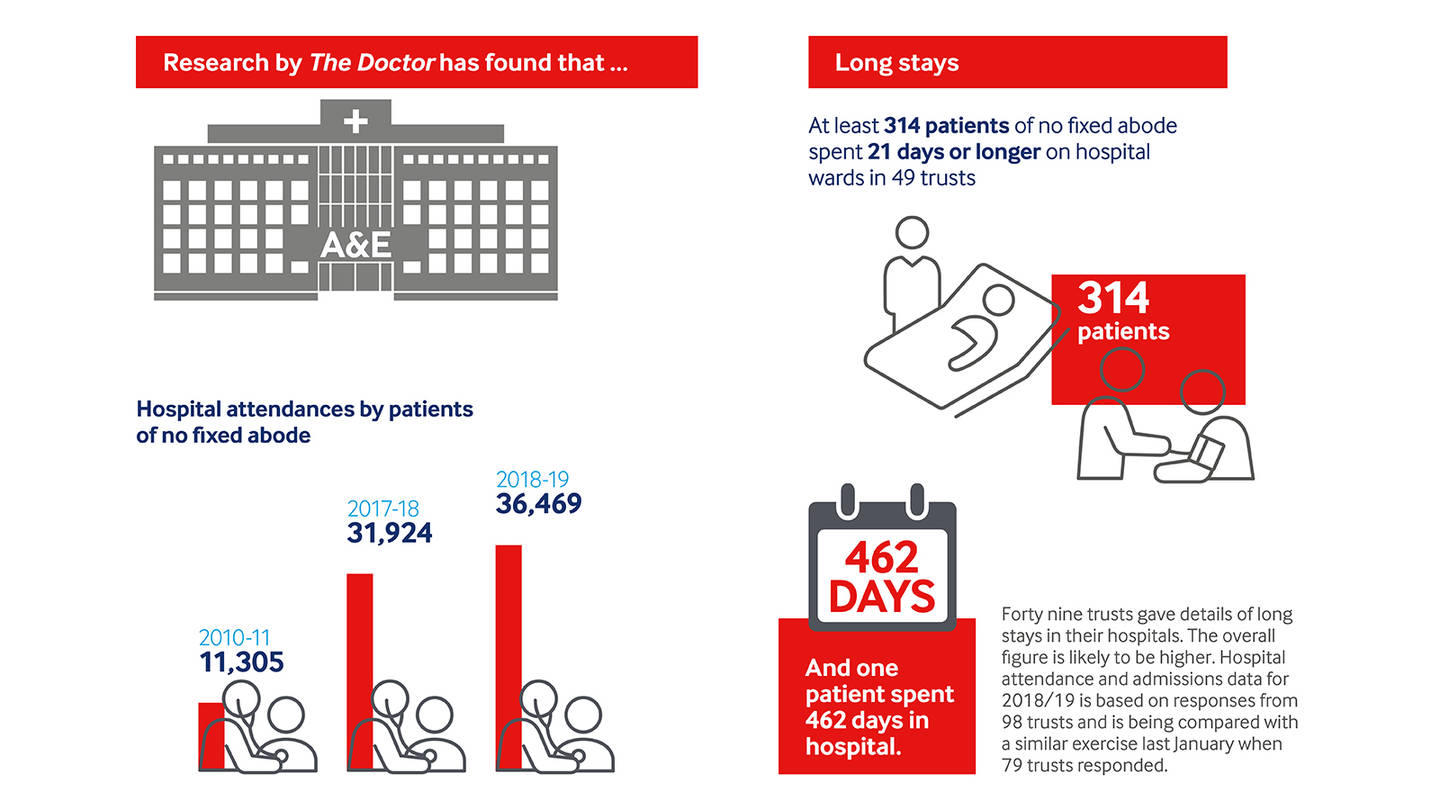
New research gathered through a series of FoI (Freedom of Information) requests responded to by the majority of trusts in England, reveal hospital attendances by patients with no fixed abode soared to at least 36,469 during 2018-19.
Those figures represent a massive rise from 11,305 in 2010-11 and a significant jump from figures for the year prior, 2017-18, which totalled 31,924, according to statistics previously collated by The Doctor. Last year alone those emergency department attendances cost the NHS at least £5.8m, at £160 each.
It is a trend echoed in hospital admissions, too. In 2018-19, 11,986 admissions for patients of no fixed abode were recorded. In 2010-11 that total number was 3,378 and in 2017-18 it was 9,282, again according to figures previously collated by The Doctor.
With the cheapest hospital admission averaging £1,603, according to NHS Improvement, this year’s bill sits at £18.7m, at the very least.
For most of these thousands of patients hospital appointments represent more crises, but for Mr Snowball things were very different.
We have had 20 people sleeping rough in the waiting room and around the hospital grounds.
Care package
When he was admitted in 2016 a member of the Pathway team at University College London Hospitals became aware of his case.
The team identifies the complex issues in a homeless patient’s life on admission and uses their expertise – whether in clinical care, occupational therapy, social care, substance misuse or a wide range of other areas – to address the problems, looking to wrap care around them while they are in a place where they can be helped. It is a simple idea which allows hospital trusts to do more than just discharge homeless patients to the streets, more than just to count the days until their next admissions.
In Mr Snowball’s case the Pathway team allowed him to access a solicitor, found temporary hostel accommodation, helped to address his health and addiction issues and eventually assisted with finding a flat. Mr Snowball’s daughter has moved in with him and he’s able to volunteer with local projects.
‘I wouldn’t have anything that I have now, without having been to hospital, without them helping me,’ Mr Snowball reflects. ‘Things have all fallen into place quite nicely. They’ve started my life rolling again and have helped me all along the way. It has just gone onwards and upwards.’
Further research illustrates just how complicated hospital discharge for homeless patients can be – and highlights a significant breakdown in the services available for clinicians to access in the community.
Long stays
For the first time FoIs were used to reveal the number of patients of no fixed abode stuck on hospital wards for ‘long stays’ – defined by the NHS as 21 days or longer.
In total 49 trusts said that at least 314 patients of no fixed abode had stayed in hospital for 21 days or more in 2018-19 – costing at least £5.4m, a deeply conservative figure based on NHS Improvement costings of an ‘excess bed day’ at £346, as the types of treatment received cannot be estimated, and many trusts would not reveal patient numbers.
In one case, in Nottingham, a patient was stuck on a hospital ward for 462 days. And 28 other patients were on hospital wards across the country for 100 days or more.
At King’s College Hospital, London, 78 patients spent long stays in hospital, totalling 4,383 days.
The reality is likely to be even bleaker than all the statistics gathered for attendances, admissions and long stays – with NHS recording mechanisms notably poor, hidden homelessness a growing issue and a number of trusts not recording data or not responding to requests for information.
In any other condition there would be horror that the average age of death in these patients is in their 40s.
Low mortality
 Barbara Cleaver
Barbara Cleaver
Faced with this sort of demand – and without the tools to cope – frontline staff are left in an increasingly difficult position, making decisions that will have a huge effect on the health and life outcomes of their patients. After all, homeless patients die, on average, in their 40s.
Barbara Cleaver, emergency medicine consultant at Imperial College Healthcare NHS Trust, says the demand and complexity of patients, combined with lack of ability to make a difference to their homelessness, is obvious on the front line.
‘There is an under-the-iceberg figure of people,’ she says. ‘We have had 20 people sleeping rough in the waiting room and around the hospital grounds – there is a sense that this is a place that is open 24 hours a day and is warm, well-lit and safe.’
Dr Cleaver adds: ‘It’s pretty difficult to feel good about doing your job when you are put in those positions or if you are making people homeless. These sorts of things are happening much more than people think.’
Stigmatised, marginalised
These are patients of great complexity. Research by St Mungo’s found that most homeless people demonstrate a tri-morbidity of physical illness, mental health problems and substance misuse. The charity found half its residents have mental health problems, 32 per cent had an alcohol dependency and 63 per cent had a drugs problem.
A report, recently published by the Centre for Health and Development at Staffordshire University, also found that homeless patients were a complex and marginalised group, were often stigmatised or mistreated in healthcare and also, possibly as a result, had difficulties engaging with healthcare.
Most striking of all is that these patients are old and frail 20 or 30 years before their time – and the system is just not equipped to deal with that, or, often, even willing to face up to those extreme vulnerabilities.
The hospitals might think it is a result because they are out of the hospital but they will come back.
Horror story
‘In any other condition there would be horror that the average age of death in these patients is in their 40s,’ says GP Peter Buchman (featured in the video below), a member of the Pathway team in London.
‘And sometimes in a busy hospital nobody really takes the time to clock some of these issues. They might only be 40 years old and there is a sense that they should be able to cope but they are frail young – these patients have the needs of 65- or 70-year-olds, they need support living and have complex needs.’
He adds: ‘The hospital admission is a real opportunity to assess these things and really investigate but it takes a lot of real pushing and often we find we need the involvement of us as clinicians to advocate for these patients. It is sometimes about winning hearts and minds.’
And not only are the patients complex but the wider environment is increasingly complex too, particularly thanks to swingeing austerity cuts and an increasingly fragmented health, social care and wider system.

Cuts to services
The Staffordshire University report says funding cuts have led to a decrease in capacity. BBC analysis last year found that £162m had been cut from treatment budgets in England since 2013-14, while drug poisoning deaths had risen from 2,734 to 3,450 in 2016. Cuts have also been seen in mental health provision and social services.
Housing is clearly a growing issue, too. In many parts of the country it is near impossible to gain access to housing. In Manchester the Pathway team reports there being ‘nowhere for patients to go’. In that city local authority staff have even seen fit to remove the ability of clinicians and managers to refer patients directly into services. All patients now must be matched through a centralised system which takes hours to apply to and removes all utility of relationship-building between sectors. Even where accommodation can be found it is very often sub-standard.
As the Staffordshire University report says: ‘Discharging to hostels and similar temporary accommodation was questioned due to the potential for an unstable environment that again did not meet the needs or expectations of individuals.’
The result – particularly without a service like a Pathway team in place – is clear. As the Staffordshire report, and so many other sources, show – patients are being discharged to the streets totally unfit for that sort of lifestyle, if indeed anyone can be fit to sleep rough.
Unstable environment that again did not meet the needs or expectations of individuals.
Lack of investment
 BMA council chair Chaand Nagpaul
BMA council chair Chaand Nagpaul
One local authority worker reflects on patients being discharged and given sole responsibility for their care – even ‘released with drains and all sorts of things that need aftercare’. The alternative is patients stuck in hospital beds, as the long-stay figures show. Neither outcome is successful, or, indeed, ethical.
Clearly there is a massive need for investment: hospital beds, proper preventive public health, social care, mental health resourcing and, hugely importantly, a genuine house building programme.
It is crucial the NHS, and indeed other related services, are put back on a ‘sustainable footing with the capacity to meet the demands’ on services, as BMA council chair Chaand Nagpaul said last month.
Integration mirage
The integration agenda could also be crucial. Pathway teams are, ultimately, multi-disciplinary, cross-service teams that bring the best skills together to wrap around the patient’s need. They display the sort of integration much of the health service only dreams about. And it appears to be effective. But integration talk is cheap – and has been on the lips of NHS leaders for years. File that one in the ‘wait-and-see’ pile.
But, until all this change is realised, it is in this environment that doctors work and homeless patients live: an environment of ever-growing demand. Here, Pathway teams come into their own, with the skills, experience and single-mindedness to try to make a difference.
Developed by the Pathway charity, the teams are generally based on a GP-led model where a small team of health professionals is integrated into a hospital trust, in a bid to help find accommodation and support for patients and avoid discharge back on to the streets.
The phone seems to ring endlessly in the office of the Pathway team at the Royal London Hospital in Whitechapel. This cramped, corridor-like room may lack the grandeur of hospital boardrooms or the military-style urgency of bed management meetings, but, here, the daily battle of the NHS in 2019 is fully displayed, albeit in microcosm, through the struggles of one cohort of patients.
Sometimes you need a bit more time in a supported environment.
Chance to help
 Pathway team at the Royal London Hospital in Whitechapel
Pathway team at the Royal London Hospital in Whitechapel
When that phone rings and signifies the presence of a new homeless patient in hospital, a team of just five staff – a GP, nurse, occupational therapist, social worker and care navigator – spring into action.
‘A hospital admission is an amazing opportunity,’ Dr Buchman says (pictured centre-right). ‘Someone is in a place where you can help them and where they may want help also. It can be an opportunity to break the cycle.’
But across the country a freed-up hospital bed is worth more than its weight in gold. As such, time is of the essence, and constant communication – and more than a hint of gentle persuasion – is often required to find a successful outcome.
Where possible, and the complex illnesses of homeless patients often mean time in hospital is lengthy, patients are assessed and their history and issues discussed, GP registration arranged, housing departments called, care packages considered and even shoes, clothing and a mobile phone found. A plan is put in place.
Further support
It is not just about people, either. The Pathway homeless team at the Royal London have access to a six-bed facility that makes a huge difference to the whole process – a step-down facility, where homeless patients well enough to leave hospital, but still needing support or time to put further plans in place, can recover. The Stoke Newington-based facility, which comes with access to a large shared kitchen and is manned 24 hours a day, makes a huge difference.
Dr Buchman says: ‘We’re very lucky to have it – there are a lot of people who there may be a solution for but with all of the frustrations of the system – navigating benefits, lost identification, the housing system and accessing services – sometimes you need a bit more time in a supported environment.’
The effects of Pathway teams and these sorts of facilities can be monumental in a patient’s life – and can have a serious, positive, impact on costs for the health service.
Smiling, Dr Buchman cites the example of a patient treated for a fractured leg, who would have been discharged on to the streets. Room was found for him at the step-down facility and it later emerged that he was the unwitting victim of modern slavery.
‘He’s heading for legal status here – he’s somewhere safe and he has the chance to move on to a more normal life. It’s an amazing transformation and just shows the opportunity you have.’

Marked improvement
The evidence base for the wider rollout of similar services to Pathway teams is as strong as the evidence of growing need.
A Pathway team operating in Brighton (which will be featured in the next issue) has had a major effect. In 2018/19 compared with the previous financial year, measuring patients registered at the homeless GP surgery, the team demonstrated a 6.1 per cent reduction in emergency care attendance, a 26.1 per cent reduction in unplanned admissions and a 35.4 per cent reduction in readmissions within 30 days.
And a study looking at 410 patients, which included the Royal London, found that the proportion of people sleeping on the streets after hospital discharge was 3.8 per cent in a cohort of patients exposed to a Pathway team, compared with 14.6 per cent receiving standard care.
It seems to echo what doctors called for at this year’s BMA annual representative meeting – the roll out of integrated inpatient homeless healthcare and wide-ranging action across the health system.
Yet there are only 11 trusts operating Pathway teams at hospitals in England.
Waiting times

Pathway clinical director and GP Nigel Hewett says: ‘We think there are about 50 hospitals that might benefit from the approach. At the current rate (of introducing the system to hospitals) that means we will have to wait another 40 years.’
Steve Wynne, senior Sister in the Royal London homeless team, says: ‘How on earth do people (without a specialist team) manage? They must be sending so many people out on to the streets. The hospitals might think it is a result because they are out of the hospital but they will come back.’
Even in a society increasingly hamstrung by growing demand – as demonstrated by the research for this piece – and contracting services, the opportunity of a hospital admission remains, according to those who know best.
And the case for putting the people in place who can make the most of that opportunity is pragmatic – the NHS needs the respite and, crucially, so do patients.
As Mr Snowball says: ‘It’s about giving people a chance – but it’s also forcing them to take the chance. Putting people around them, giving them the help they need. There are ways to get people off the streets and get their health going again, but you need to give people a push when they need that help.’