
‘I remember it really well. It was September 2019, before COVID hit, and we had got to something like 50 people OOA [out of area] on our worst day and it was just creeping and creeping. It got to a point where we just thought, this is not acceptable and we’ve got to do something.’
Samantha Wood is head of service for mental health, inpatients and urgent care services at Leicestershire Partnership NHS Trust, the organisation responsible for mental health services in one corner of the East Midlands.
She recalls the moment of reckoning which forced action – the beginning of a process which has seen her trust massively decrease the number of vulnerable mental health patients sent miles away from home, instead looking after them in their homes, communities and local hospitals.
Ms Wood says a patient flow team was created, to be led by her and head of nursing Saskya Falope. Their efforts to drive change were soon accelerated by the effects of COVID-19 where, suddenly, across the health service, bureaucracy went out of the window and transformation and innovation were encouraged – even rushed through – rather than stifled, as is so often the case.
‘We were given permission to try things out,’ consultant psychiatrist Samantha Hamer says.
It got to a point where we just thought, this is not acceptableDr Hamer
The team was able to set up an urgent mental health hub where patients could be seen in a much calmer environment than an emergency department and with more direct access to the specialists they required.
Dr Hamer and her colleagues feel this approach allows patients to be treated in environments more suited to their care and relieves pressure on services which are crumbling in the face of rocketing demand – with patients who could be treated better elsewhere, not automatically taken into acute services and clinicians given headroom to make the best decisions about admissions and discharges.
The hub, the team say, comes without the immediate pressures of turnaround targets in an incredibly busy and stressful emergency department setting.
‘It can take longer to ensure they have the right support and the right assessments, but you don’t have to just say: let’s admit because we’re stuck here.
'That’s been really helpful,’ Dr Hamer adds.
On top of this they set up a community-enhanced rehab team with money clawed back from the costly practice of sending patients to private hospital beds OOA.
There are other useful tools, too, such as the use of a crisis house and a system where healthcare professionals directly access the ambulance call stack to divert resources and patients to the right places.
We were given permission to try things outDr Hamer
The team’s work came in recognition of a problem which was becoming overwhelming in Leicestershire, like much of the country.
Each month, significant numbers of patients were being sent miles away from home to costly private hospital beds due to a lack of capacity in the system and relentless, increasing, demand in communities.
The use of OOA beds, doctors agree, is a poor solution for both patients and the health service with vast amounts of money leaving the NHS and patients left isolated away from support networks.
Data, published by NHS England, showed that 380 patients were sent OOA inappropriately during January 2023 alone. Of those patients, 59 per cent were placed more than 100km away from home and 46 per cent were on those hospital wards for more than 30 nights.
Almost all these beds are run by private firms and come at a significant cost to the NHS.
Not all of the progress comes from improving services or improving patient pathways, however. The team is quick to credit increased communication with partner organisations, a change of culture and a sense that everyone is in it together.
During COVID, staff from the trust set up weekly meetings with all the relevant representatives from local authorities, charities and social care providers and each patient who needed a hospital bed or needed discharging was discussed in detail.
For the first time it crystallised the sense that these individual cases were real people, not easily thought of as numbers, Ms Wood says.
Dramatic improvement
The enthusiasm of the team is abundantly apparent, and it appears their efforts are having a real effect. Figures released to The Doctor under the Freedom of Information Act suggest the trust initiated 162 ‘inappropriate’ OOA placements in 2017/18 followed by 168 the following year.
In stark contrast, the most recent annual total – the trust now reports in calendar rather than financial years – was just two. Dr Hamer says: ‘Overall we’re really pleased because it does mean we are not sending patients miles away.’
It is an achievement which will likely make a big difference to the lives, and recoveries, of patients as well as to the wellbeing of staff and the finances of the organisation, with private OOA beds often very costly.
There are still significant challenges for staff in Leicestershire, not least with access to social care packages and housing increasingly difficult, and ambitions for mental health trusts to have bed occupancy levels of 85 per cent while keeping patients in house.
The efforts to drive change in Leicestershire are in line with progress the Government promised to make – pledging to end the practice of OOA placements by the end of March 2021.
However, in the April issue of The Doctor we revealed that vulnerable patients with mental health conditions are still being sent hundreds of miles away from family and friends.
 ELDRED: OOA placements have a negative effect on staff and patients
ELDRED: OOA placements have a negative effect on staff and patients
James Eldred, a consultant psychiatrist in the south-west of England, identifies the effects of isolation on patients, the potential for degrading relationships between clinicians and patients and families, and the strain on staff trying to communicate with unfamiliar organisations and keep tabs on patients all around the country.
He says patients can feel ‘unwanted’ and staff ‘demoralised’ by a problem they often feel is spiralling and getting ‘away from them’.
BMA consultants committee mental health lead Andrew Molodynski adds: ‘Being put in the back of a locked ambulance and transported to somewhere you’ve never heard of is traumatising, distressing and scary.
'While there are some occasions when patients need specialist treatment, and local systems are overly pressurised, that this situation is endemic despite the current chancellor pledging to end it while he was health secretary clearly shows this Government does not value these incredibly vulnerable people enough.’
 MOLODYNSKI: Government does not value vulnerable people enough
MOLODYNSKI: Government does not value vulnerable people enough
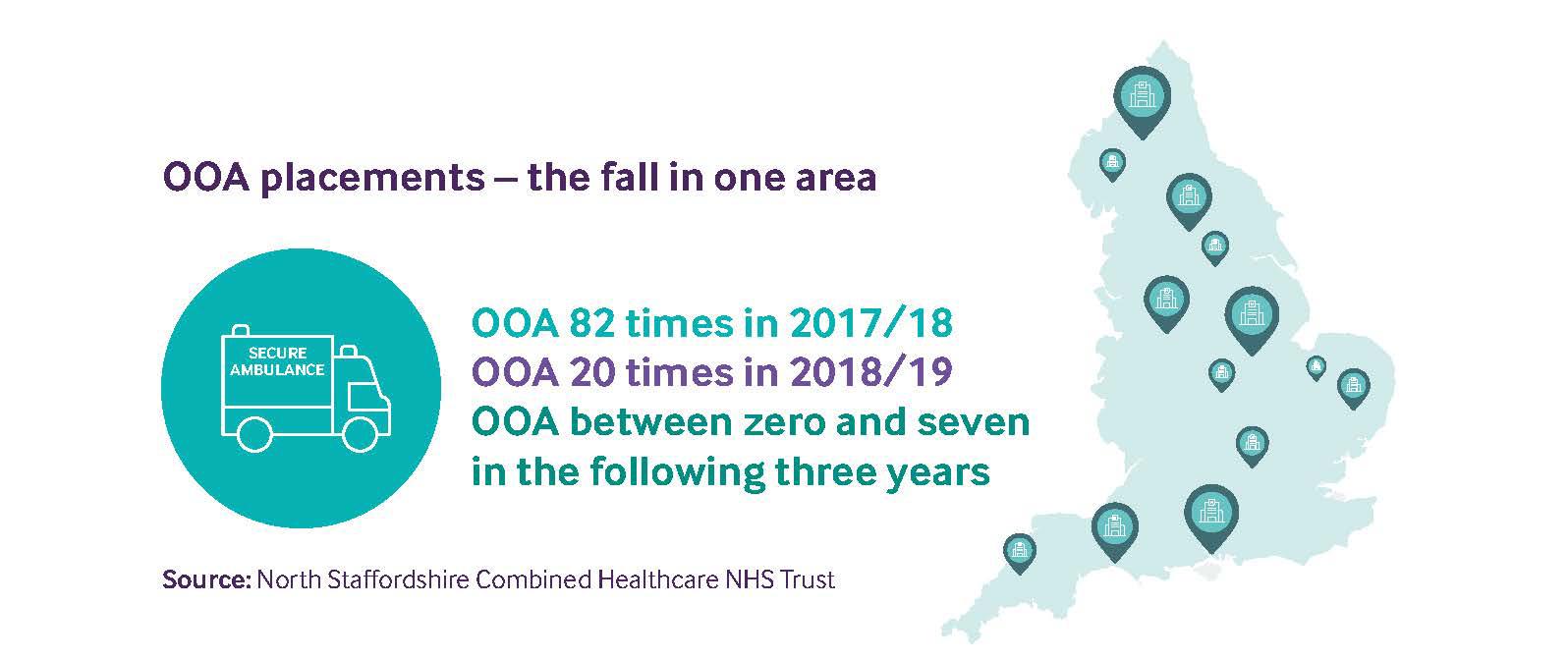
North Staffordshire Combined Healthcare NHS Trust is one of the few organisations around the country which provided figures showing a significant drop in ‘inappropriate’ OOA placements to The Doctor.
The statistics suggest that the trust placed patients OOA 82 times in 2017/18, but that number decreased to 20 the following year and has not been above single figures for any financial year since.
Dennis Okolo, the chief medical officer for the trust, says the organisation has always been keen to ‘prevent’ and ‘reduce’ admitting patients to private beds miles away and has put a lot of initiatives in place locally to avoid doing so.
Many of the projects Dr Okolo describes will be familiar to doctors across the country but, in a package, together, they are helping the team to avoid use of OOA placements.
Dr Okolo says all patients who have been deemed to require a bed automatically go to the trust’s home-care team to justify their need for that bed and to ensure they cannot be cared for in their own environment.
 OKOLO: Close working between agencies boosts efficiency
OKOLO: Close working between agencies boosts efficiency
Beyond that Dr Okolo says on-call doctors are encouraged to be part of assessments because they are more likely to know and understand patients and can make decisions with greater clarity.
He also identifies intense reviews of discharges, close work with local authorities, the liaison psychiatry team in the local emergency department, high-volume service user focus, having a strong personality disorder service, and a local psychiatric intensive care unit, as among the reasons for being able to manage demand efficiently.
Despite the moments of success, areas such as Leicestershire and North Staffordshire have reported there remain significant concerns for the future – in those areas and across the country.
The first piece in The Doctor’s Paucity of Esteem series – published in March – revealed massive increases in demand and pressure across the mental health system, and huge rises in the number of mental health patients presenting at emergency departments in crisis and being trapped there for days or even weeks as a result of the pressure on, and state of, services elsewhere.
The Government does not value these incredibly vulnerable people enoughDr Molodynski
Doctors fear pressures are only likely to get worse owing to the cost-of-living crisis, the fall-out from the pandemic and the effects of austerity politics.
The Doctor has spoken to a wide range of mental health professionals and experts across the country while producing the Paucity of Esteem series and suggestions to tackle the issue of OOA placements have been varied.
All, however, unanimously agreed that the workforce is an urgent issue with huge numbers of vacancies and a growing sense of burnout among those in position.
The BMA is urging the Government to expand the number of inpatient mental health beds in England so NHS England can finally meet the missed target to eliminate inappropriate OOA mental health placements.
The association is also supporting the Royal College of Psychiatrists’ recommendation that all new integrated care partnerships conduct service-capacity assessments and target investment towards services driving inappropriate OOA placements locally.
As Dr Eldred says, OOA placements are not a ‘healthy thing from anyone’s point of view’.