
Kierran Fletcher, a father and professional Thai kickboxer in his 20s, had been waiting, bags packed, for 24 hours for a hospital bed when he rushed out of his home and killed Nigel Abbott in a frenzied assault, believing him to be the devil.
Mr Fletcher’s first episode of psychosis had been diagnosed quickly by his GP the previous afternoon. Hours later, an urgent admission had been advised by a psychiatrist. After considerable effort, his family had persuaded him to be treated.
But there were no beds free in BSMHFT (Birmingham and Solihull Mental Health Foundation Trust) on that night, 26 July 2018. Mr Fletcher instead joined a queue with 23 other seriously ill patients.
This mental health service, for more than a million people, lacked section 140 beds, a supply backstop which every part of the NHS has been required to have ready for such urgent cases since the Mental Health Act became law in 1983.
While waiting, the care of Mr Fletcher was handed to one of the trust’s five HTTs (home treatment teams). At that time, they were struggling with up to double the caseloads they could carry and vacancy rates as high as 95 per cent.

 CRIME SCENE: The street in Sutton Coldfield where Mr Abbott was attacked
CRIME SCENE: The street in Sutton Coldfield where Mr Abbott was attacked
As Mr Fletcher’s condition deteriorated on the day and evening of the attack, his family called his HTT 60 times.
Very few calls connected. There were still no beds at 8pm, his family heard on the last call answered, hours before Mr Abbott was assaulted and killed, as he walked to the pub. Mr Fletcher was later found not guilty of murder by reason of insanity.
This wasn’t the first time England’s second largest city had run out of room and it won’t be the last in Birmingham, Solihull, or much of England, an investigation has found.
The Doctor found that the pressures and risk factors pinpointed by Birmingham and Solihull coroners in this and 10 other deaths which they have examined are present in much of England. The Doctor found waiting times for beds running into weeks, high vacancy rates in HTTs nationwide, and no section 140 backstop supply in much of the country.
The findings reinforce further a point the BMA and other medical bodies have been raising for some time: there simply aren’t enough mental health beds in much of England.
A consultant psychiatrist and clinical director at BSMHFT, whose name is redacted in inquest papers, called mental healthcare in the city ‘broken’ for its ‘weak and incompetent leadership’.
Staff there felt ‘helpless’; they had learned there was ‘no point’ in asking for beds. Its chief mental health legislation officer, a consultant forensic psychiatrist, said services were in ‘massive crisis’ in 2018. ‘Deaths are occurring in Birmingham because of a lack of resources,’ they added.
Unsafe waits
The investigation indicates that such sentiments are likely felt by frontline staff elsewhere.
As is depressingly common in mental health care, most trusts appear unaware of their risks of prolonged waiting times for beds. They just don’t record them.
The Birmingham and Solihull coroners linked 11 deaths in their area in the space of one year to prolonged and fruitless searches for beds. Anthony McCormack, the most recent, took his own life in May 2019, after the longest wait of over a month.
‘Suicide due [to] unavailability of an inpatient mental health bed,’ was the inquest’s conclusion. Anthony Watson died also from suicide in October the previous year, aged 72, after waiting three days, the coroner found.
Despite the risks linked to waiting times, the vast majority of mental health trusts, including BSMHFT, do not record them, according to the 36 FoI (Freedom of Information) responses The Doctor received. Just six did last year; they reported waiting times of up to 29 days.
Hundreds of patients waited more than three days for a bed last year, figures from just four trusts show. More than 1,300 waited more than 24 hours – the average wait for patients of Rotherham, Doncaster and South Humber Mental Health NHS Foundation Trust.
Multi-factored assessment
The way risks accumulate as acutely unwell patients wait at home for a bed is laid bare in the Birmingham and Solihull coroners’ reports.
They show how admitting patients with acute mental ill health often requires the coordination of multiple public bodies, such as the NHS, police and ambulance services, and local authorities.
Each one brings into the mix their own pressures and ways of doing things. In Mr Abbott’s case, the ‘ambiguous wording’ of one ‘multi-agency memorandum of understanding’ stopped staff from calling police for assistance. ‘They anticipated the police would be too busy,’ the coroner’s report says.
In mental healthcare, admissions are supposed to be coordinated with a ‘clear, joint policy’ agreed by all agencies involved, according to the Mental Health Act code of practice. Yet only four of the 100 CCGs (clinical commissioning groups) which responded to The Doctor’s FoI, knew of such coordinating policies.
Without an agreed way of working together, the potential for confusion and delays mounts as hour-long waits turn to days. It’s magnified further in the NHS when mental health teams are pressured, understaffed, or reliant on agency workers who are less familiar with arrangements than permanent staff.
Deadly delay
In Mr Fletcher’s case, he was not prioritised for a bed after his first assessment, the night before the attack, as he should have been.
Ten hours passed before an official referral reached the AMHP (approved mental health professional) service for a full Mental Health Act assessment – at 10am, the following morning.
The AMHP’s lunchtime call to the HTT was returned three hours later, at 3.35pm. Towards the end of the day, Mr Fletcher’s case was closed incorrectly by his AMHP.
‘Longstanding frustration with the challenging environment,’ was the reason she gave at inquest. A second referral had to be made, at 6.01pm.
Deaths are occurring because of a lack of resourcesBSMHFT staff
At 8.06pm, just under three hours before the attack, a bed was still yet to be found.
This pressure on staff working in ‘under-resourced’ teams was pinpointed as a risk by coroners in most of the 11 cases they examined.
‘The HTT, bed managers, and AMHP services are operating caseloads significantly beyond their recognised capacity,’ says the report into Mr Abbott’s death.
Adding to this pressure was BSMHFT’s recruitment problem. All five of its HTTs had unfilled posts at the time of Mr Abbott’s inquest, including in management positions, the inquest heard. The caseload of the HTT in charge of Mr McCormack’s care was five times the size it could handle. He too had been taken off the waiting list for a bed.
No backstop beds
The investigation shows that many other HTTs across England suffer significant difficulties recruiting permanent staff, albeit not on the same scale as in BSMHFT.
Vacancy rates in one of its teams hit 95 per cent in the year Mr Abbott was killed, the trust’s FoI response says.
The Doctor found that almost half (48 per cent) HTTs or their equivalent have struggled with vacancy rates of double the national average in the past three years.
Camden and Islington NHS Foundation Trust says it is addressing high vacancy rates after seeing them rise in one of its teams from 15 per cent in 2017/18 to 32 per cent last year.
Fifty-eight per cent of posts in Dorset Healthcare University NHS Foundation Trust’s connection team were unfilled last year. The average vacancy rate in England for medical and nursing staff is 10 per cent.
In Birmingham and Solihull, many posts in its HTT were unfilled, in part, for the ‘unattractive working conditions’, frontline staff told the coroner.
Services are operating caseloads significantly beyond their recognised capacityReport into Mr Abbott's death
But perhaps the starkest finding of the investigation is the widespread lack of section 140 backstop beds in the NHS.
Section 140 of the Mental Health Act requires all CCGs to have arrangements for beds in urgent situations.
Birmingham and Solihull CCG had been chased for four years to put them in place by the consultant forensic psychiatrist who gave evidence at Mr Abbott’s inquest, the coroner heard.
Concerns about the lack of section 140 arrangements nationally have been raised by the CQC (Care Quality Commission) repeatedly, and by consultant psychiatrist Professor Sir Simon Wessely in his review of the Mental Health Act in 2018. More recently, in May 2020, NHS England urged mental healthcare ‘systems’ to get them in place in anticipation of additional pressures from COVID-19.
Lack of arrangements
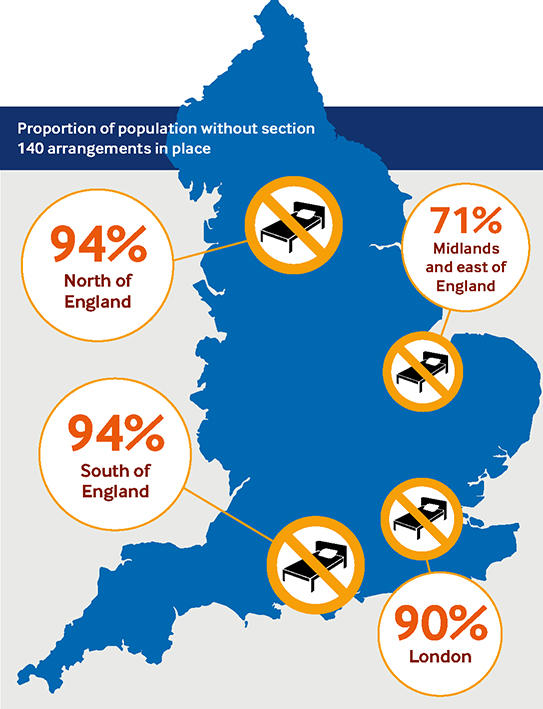
The investigation has, however, found that vast swathes of the population of England, some 33 million people, live in areas where their CCGs could not point to their policies for these backstop beds.
Of the 100 CCGs which responded, only 12 said they could point to one in place. Six had one in draft. While most CCGs said arrangements were in the hands of the mental health trusts they commissioned, the NHS and the MHA code of practice is clear that they must be involved. Birmingham and Solihull CCG now has a policy for section 140 beds, it confirmed in its FoI response.
Available beds at BSMHFT have, however, decreased since the coroners’ intervention, as the number of patients it sends to other hospitals ‘out of area’ soared by 161 per cent since 2018, the year Mr Abbott was killed. ‘Extremely concerning’ levels of patients waiting for beds have been reported at the trust as recently as October in the trade publication, the Health Service Journal.
Birmingham and Solihull CCG has no plans to increase its ‘bed stock’ in the next three years, its FoI response says.

The CCG had been ‘unable to validate a link between funding and the deaths’, NHS England told Birmingham and Solihull coroners in its response in 2019. In a joint response with the trust, Birmingham City Council, and the West Midlands Police, the CCG says it had in fact ‘exceeded’ the NHS ‘mental health investment standard’ since its inception.
A spokesperson for BSMHFT says: ‘In light of both increasing demand, and the complexity of patients’ needs we are working hard with our partners to create a mental health system that addresses the demand and capacity issues we are facing.’
It had invested in its HTTs, improved support for crisis cafés, set up a 24/7 mental health helpline, and planned next summer to open a new urgent care centre. ‘This will mean a more timely and joined-up assessment process and fewer delays for people who are experiencing a mental health crisis.’
Legal requirement
As The Doctor reported in November, bed numbers in many areas of England are expected to fall as demand rises, fuelled by the effects of COVID-19. ‘Severe stresses in bed management’ were predicted in November by the CQC in its annual monitoring report on the Mental Health Act.
Without section 140 arrangements, much of the country lacks even the emergency backstop required by law. Struggling – sometimes unable – to keep patients safe at home are the community mental health teams, burdened by ever-increasing caseloads.
The battle for more resources from frontline staff might be an old one but it’s one which looks set to grind on for some time in Birmingham, Solihull, and much of England. The awful outcomes for patients and their families will be told by coroners again, until somebody listens.
How much more tragedy will it take?
Seriously ill patients are being kept from safe beds and treatment until it’s too late, with severe shortages of staff to treat them, says consultant psychiatrist Andrew Molodynski

As a society, we should applaud Birmingham and Solihull coroners for pinpointing the risks which arise when mental health services are under-resourced, under strain, and understaffed.
They’ve shone a light into a dark and dank corner of the NHS, they’ve exposed our leaders’ attitudes towards people in mental health crisis. They’ve found multiple reasons which could have prevented another life lost, another family being hollowed out. They’re reasons which will be wearily familiar to many frontline staff in other parts of the NHS.
Despite the rhetoric from politicians and, worse, from those who provide and commission services, patients at severe risk to themselves or others are still being kept waiting for days, weeks, even more than a month for hospital beds. If that’s not bad enough, we found that most of the NHS does not record this data.
The confusing and complicated ‘arrangements’ (one could not call them systems) that open up gaps between police, social workers, and NHS teams are causing distress, infringing human rights, and costing lives. Many home-treatment teams, those expected to reduce hospital admissions in the NHS Long Term Plan, are buckling under workloads. Many run on agency staff, with vacancy rates as high as 95 per cent.
There isn’t even the backstop of section 140 beds in many areas, despite this being repeatedly flagged by national bodies, reviews, and no doubt individual doctors, as in Birmingham and Solihull.
Politicians and senior NHS managers are in collective denial. Frontline staff, carers, and those who use services are not, but their voices are not being truly heard. The Government must do more to address these concerns, including meeting with key representative bodies, including the BMA.
These tragedies happening up and down our country involve people with one characteristic in common: mental ill-health.
This has now become a civil rights issue, with a group of people identifiable by a particular and definable characteristic being allowed to suffer and let die for want of decent, affordable care.
How many more people need to die before things change?
Andrew Molodynski is BMA consultants committee mental health policy lead